
A new framework for health equity leadership lays out the key skills and conditions necessary for success.
The Institute for Healthcare Improvement published its Defining the Health Equity Officer Role report, based on learnings from a related rapid-cycle innovation project as well as an advisory group of health equity officers. The framework provides the basis for IHI’s Leadership for Health Equity Professional Development Program, which starts in September. It also builds on prior IHI frameworks, including Achieving Health Equity and Organizational Trustworthiness in Health Care.
Over the past several years, as the pandemic exacerbated long-standing inequities, many hospital systems began to hire leaders to help achieve and sustain institution-wide health equity goals. However, given that the role was mostly a new phenomenon, those leaders did not have a blueprint for doing the work—a gap that IHI aims to fix with its report.
The latest framework comes at a time of heightened perception that industries across the board are moving away from work in diversity, equity and inclusion.
“DEI conceptually has become a political concept and there is an aversion to it, particularly from the right,” Kedar Mate, M.D., president and CEO of IHI, told Fierce Healthcare. “Perceptions are based on some evidence, but I don’t have objective information to support this.”
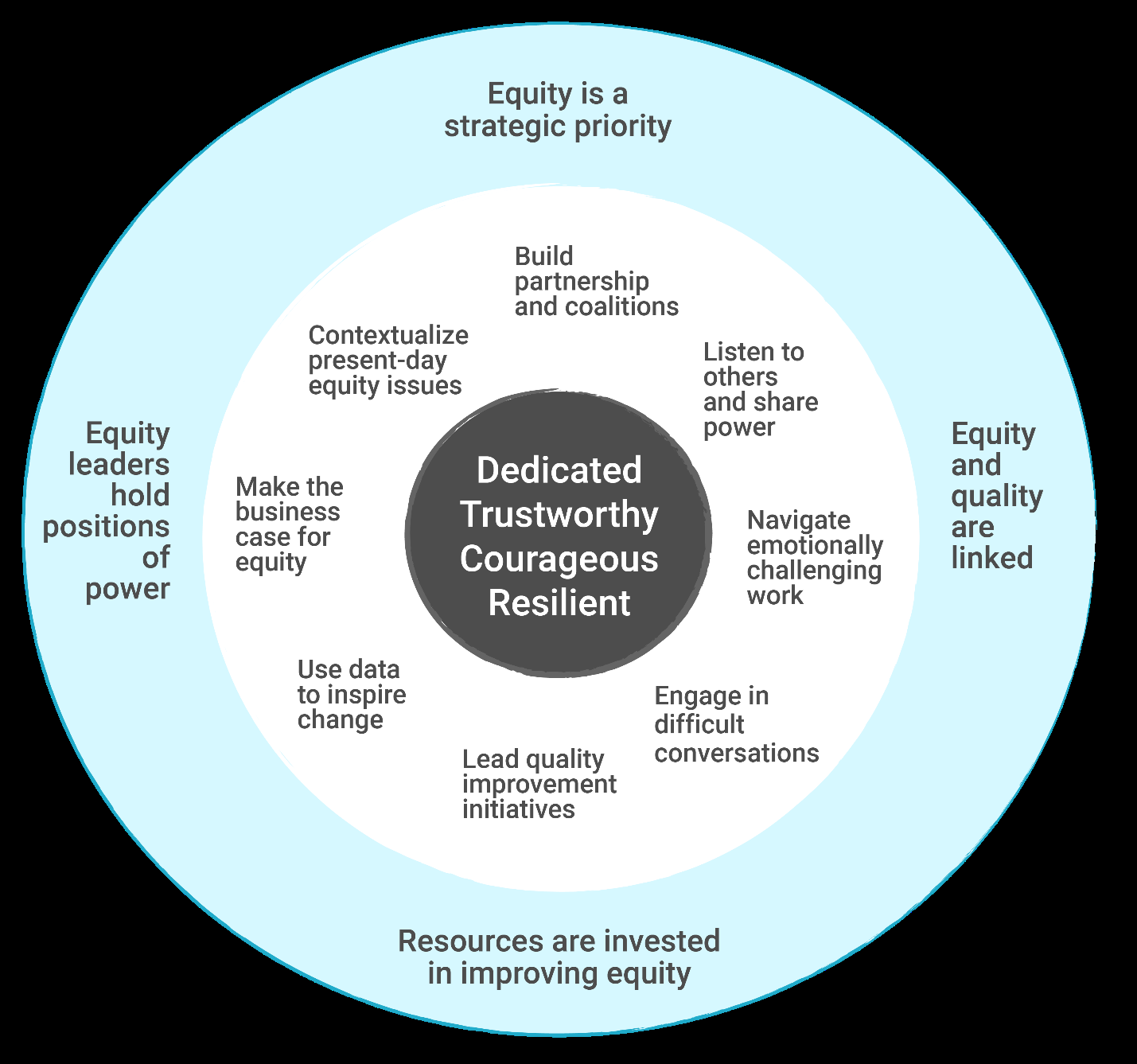
Credit: Defining the Health Equity Officer Role report via the Institute for Healthcare Improvement
At the center of its framework are core ways of being: dedication, trustworthiness, courage and resilience. Dedication involves being committed to equity and anti-racism, while trustworthiness is made up of integrity, humility and leading with love and humanity.
From there, the skills worth having include contextualizing present-day equity issues and analyzing mindsets, actions and systems that uphold inequities. Leaders should be prepared to lead quality improvement initiatives and use data to inspire change.
Leaders should also be prepared to build partnerships, listen well and be comfortable sharing power.
“There’s no other way to get a better understanding of what the inequalities are or what’s driving the inequities in the system,” Mate said. “So much of what drives inequities has to do with how communities perceive healthcare.”
“There’s ways in which you have to learn to work with community and do community engagement in a way that is not harmful,” Camille Burnett, RN, IHI’s VP of health equity, previously told Fierce Healthcare at the 2023 IHI Forum. “You can’t just jump in and say I’m here, let’s do this—you have to share power, you have to co-create,” she said.
Leaders are also expected to be able to navigate difficult conversations about racism and have emotional intelligence on the job in order to move toward progress. And leaders should make the business case for equity, for instance by linking it to metrics that are already strategic priorities.
While there is also a strong moral argument to be made for doing equity work, the business case might appeal more to a specific audience, such as a hospital board. Good leaders will distinguish which to present when, per Burnett: “It’s having them socialize what that might sound like and being able to make it very unique for their organization.”
“My view is that each of the arguments has merit and standing and value on its own,” Mate said.
Finally, the last part of the framework names conditions for success, of which there are several: bold leadership, governance, resources and structure.
First, equity must be a strategic priority across the organization, with support from senior leadership and governance boards. Organizations should also be armed with language and data to answer questions about what success in health equity looks like, and acknowledge that this work is going to be long-term and complex.
Second, equity leaders must hold positions of power to be successful, reporting directly to the CEO. This will enable progress and keep appropriate parties accountable. When an equity leader reports to the CEO, the importance of equity and its centrality to the overall mission of an organization is emphasized. Mate suspects that today, most equity officers do not report directly to the chief executive.
Third, resources must be invested in improving equity, including a broader equity team and budget. Several equity officers interviewed by IHI reported not having enough resources to achieve their vision. Ensuring these resources can also appeal to a wider range of candidates.
Finally, equity and quality must be linked. Without equity, there can be no quality, the report argued. When examining quality metrics, stratifying data may reveal disparities. These should be treated as low-quality care, just as patient safety is seen as a quality issue.
Today, organizations stratifying their data by race and ethnicity is “far more common practice” compared to just a few years ago, per Mate: “Now it is the norm that health systems have done some stratification work entering the collaborative.” Part of that is being driven by federal agencies increasingly expecting this type of collection, he added.
“We are in a moment of opportunity,” the report concluded. “As organizations commit to seriously pursuing equity through the hiring of health equity officers, it is important that the role is defined and that expectations are made clear.”